Different options are available for prenatal aneuploidy screening in twin pregnancies. To date, there are insufficient data to recommend a specific method of screening. Acceptable options are (1) screening by first trimester nuchal translucency and maternal age; (2) first trimester nuchal translucency and maternal age combined with serum biochemistry.
Down syndrome risk adjustment in twin or multiple pregnancies is complicated, since it poses complex practical and ethical issues. Zygosity, rather than chorionicity, determines the degree of risk and whether or not the fetuses may be concordant or discordant for chromosomal anomalies.
In monozygotic pregnancies, both twins are either affected or unaffected, with very rare exceptions, while in dizygotic pregnancies, the risk of aneuploidy for each twin is more or less independent of the risk for the other.
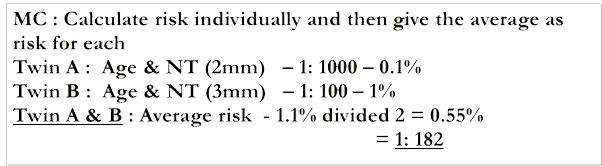
In monochorionic twins, each fetus has the same risk of being affected with Down syndrome, and the overall risk is the same as in a singleton pregnancy. Thus, the NT measurements are averaged to calculate a single risk estimate for the entire pregnancy using published NT values for singletons.
Each fetus in a dichorionic twin pregnancy is considered separately. Since each fetus has an independent risk, risk calculation in dichorionic twin gestations can be done as a fetus-specific risk.
When screening is done by nuchal translucency and maternal age, a pregnancy-specific risk should be calculated in monochorionic twins. In dichorionic twins, a fetus-specific risk should be calculated.
First trimester serum screening combined with nuchal translucency may be considered in twin pregnancies. It provides some improvement over the performance of screening by nuchal translucency and maternal age by decreasing the false-positive rate (SOGC guideline 2007).
Second trimester serum screening in twins leads to a high false-positive rate (about 10%) for a detection rate of 50% to 70%, depending on the number of markers used and the chorionicity and is not recommended(SOGC guideline 2007).
- Establish chorionicity
- Monochorionic twins are assumed monozygotic - identical risk for each fetus
- Dichorionic twins - separate risks for each fetus.
- Second trimester serum markers alone - less accurate than that in singleton pregnancies.
- For triplets and higher multiplies - risks based on ultrasound markers alone (NT based risk).
- Vanishing twin with no fetal pole - Proceed with combined first trimester screening.
- Twin pregnancy with reduced fetal pole seen - Only Age +NT based screening.